



Breast Cancer Treatment Guidelines
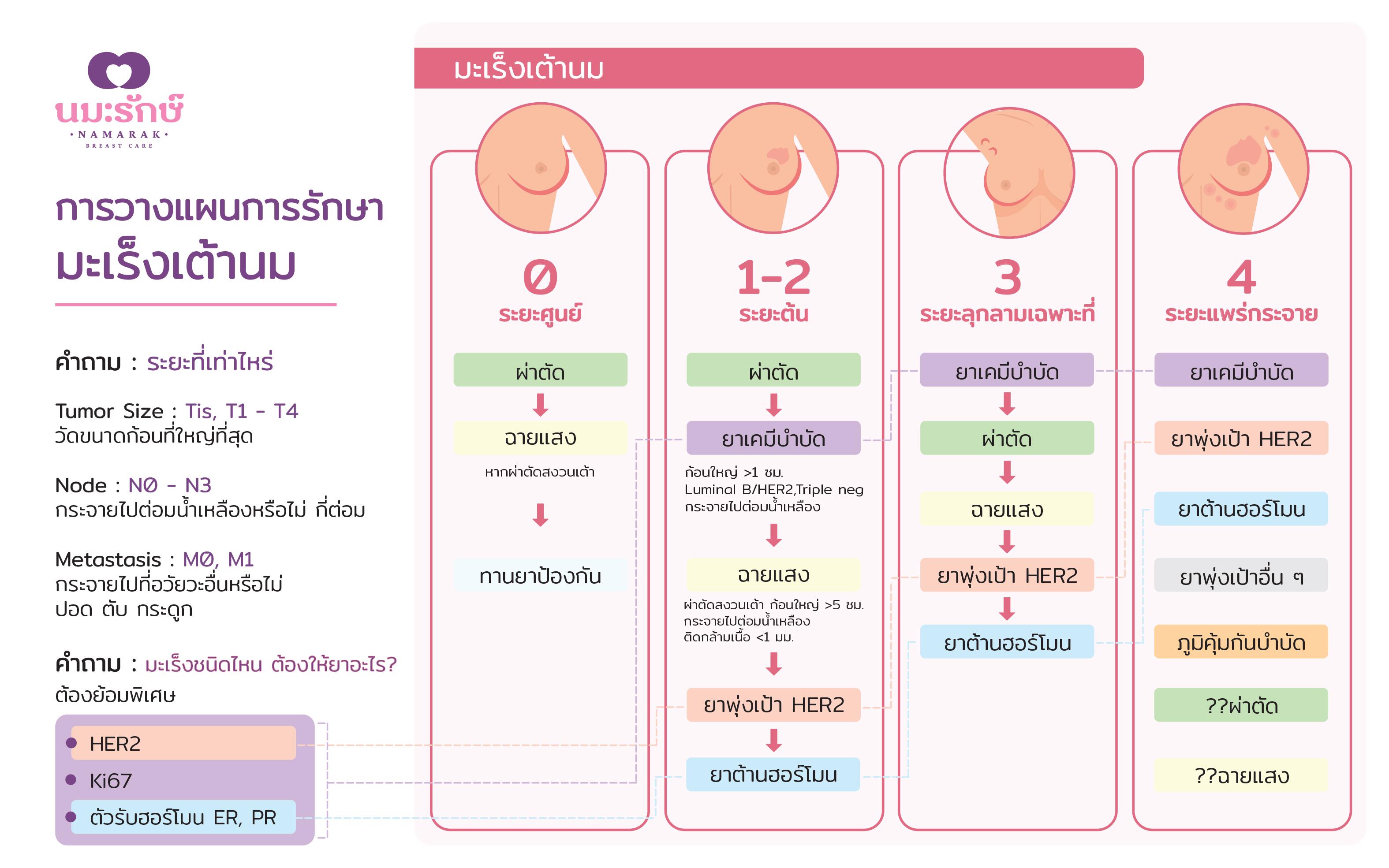
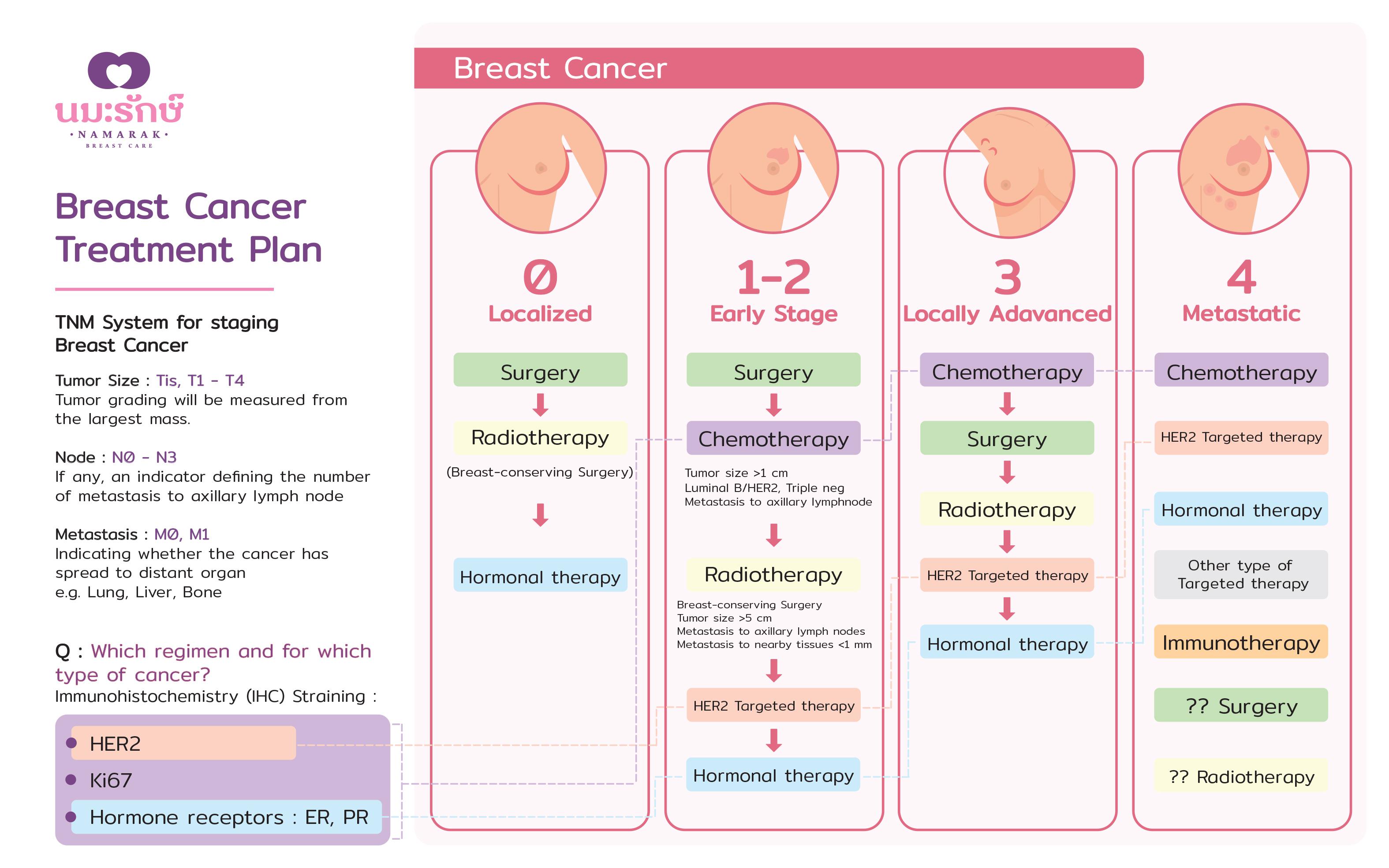
When breast cancer has been diagnosed, treatment guidelines may vary depending on the stage and type of the cancer. Breast cancer staging requires these three key factors:
· The extent of the tumor; measured from the largest mass.
· The spread to nearby lymph nodes
· The spread to distant organs.
Once all these factors have been determined, you will know the stages of the breast cancer which is usually expressed as a number on a scale of 0-4. Treatments will be administered based on the stages as follow:
Stage 0
Stage 0 breast cancer is a cancer that has not spread outside of the mammary glands or from its origin site. The chances of it spreading to the lymph nodes are only 1-2%. Thus, if proper treatment has been given at this stage, chances of being cured are more than 98%. The main treatment for this stage of cancer are surgery and other treatments which are as follow.
1. Breast surgery
There are two main types of surgery to remove breast cancer, which are Mastectomy, the removal of the entire breast and Breast-conserving surgery (BCS). If you had BCS, radiation is required on the breast where the cancer was removed to help prevent it from coming back in that area and give an effectiveness as close as the removal of the entire breast. For those who consider having a mastectomy may also have the option for breast reconstruction at the same time to restore the breast’s appearance after surgery.
2. Axillary lymph node dissection (ALND)
Since the stage 0 of breast cancer is very early, the chances of it spreading to nearby lymph nodes under the arm is only 1-2%, therefore extensive ALND is still not necessary. During the breast cancer surgery, the surgeon finds and removes the first lymph node(s) to which a tumor is likely to spread to avoid lymphedema, or the swelling of the arm.
3. Hormonal Therapy
Hormone therapy prevents and reduce the risk of cancer spreading to the opposite breast. Research has shown that Tamoxifen and Anastrozole can reduce the risk of breast cancer in women at high risk by up to 40%.
Early Stage Breast Cancer (Stage 1 and 2)
In early stage of breast cancer (stage 1 and 2), these breast cancers are still relatively small, usually not larger than 5 cm and either have not spread to the lymph nodes or have only a tiny area of cancer spread in the sentinel lymph node of not more than 3 glands. Most importantly, it has not spread to other organs. Surgery is a key component in treating breast cancer at this stage while other forms of treatments are secondary.
The doctor will use data derived from stages and variations of cancer to construct an optimum treatment plan. Further diagnostics and classification include immunohistochemistry staining, a special dyeing technique to the tissue sample to identify Estrogen Receptors (ER), Progesterone Receptors (PgR), HER2 gene and Ki-67, to measure the cancer cell division rate. These data will further be grouped again to determine the variation of the cancer which could be Luminal A, Luminal B, HER2, or Basal like (Triple Negative).
Treatment Guidelines to Early stage Breast Cancer
1. Surgery for breast cancer
Surgery for breast cancer is divided into two parts: breast surgery and sentinel lymph node biopsy (SLNB) or axillary lymph node dissection. There are several ways to perform a breast surgery, such as Breast-conserving surgery (BCS), total Mastectomy, Nipple-sparing mastectomy with reconstructive breast surgery etc. As for SLNB, during the breast cancer surgery, the surgeon finds and removes the first lymph node(s) to which a tumor is likely to spread as necessary to avoid lymphedema, or the swelling of the arm. Due to its early stage, the likelihood of the cancer spreading to the lymph nodes is approximately less than 20%. In lymphatic mapping, a surgeon injects a radioactive substance called Iso sulfan blue, then make a small incision to trace the first lymph node that are stained with the blue dye with the naked eye. Some institutions may also use diagnostic radiopharmaceuticals to provide a more accurate detection. This technique requires radioactive injections and tools to detect the lymph node(s) with radiation. At present, there is a new technology that administers the Indocynine green radioactive substance and uses a Near field Infrared Fluorescence imaging to detect the lymphatic and lymph nodes, upon incision. This gives a high-accuracy detection and avoid wide incisions.
2. Chemotherapy
Chemotherapy is an adjuvant therapy which is indicated to patients in the event of detecting the spread of cancer to the lymph node after surgery, and or in cases with no detection to the lymph node but the tumor is greater than 1 cm. Breast cancer groups such as Luminal B, HER2 and Basal-like (Triple negative), which can be known from the special dyeing technique of Estrogen Receptors (ER), Progesterone Receptors (PgR), HER2 gene and Ki-67, are likely to benefit from chemotherapy and prevent the recurrence of cancer rather than depending on the surgery alone. The optimal time for chemotherapy is 4-8 weeks after surgery. The chemotherapy regimen varies, usually 4, 6, or 8 times and is administered every 3 weeks.
3. Radiotherapy
Adjuvant radiotherapy is administered to those patients who have undergone breast-conserving surgery and postmastectomy patients with tumor greater than 5 cm, or the cancer has spread to the lymph nodes, or margin close to normal tissue such as the muscle behind the breast. Radio therapy should be administered six months after surgery with the session lasting for 4-6 weeks.
In addition to the external beam radiation, today, in modern technology, intrabeam or the intraoperative radiotherapy takes about 30 minutes. This single definitive treatment is suitable for patients who undergone breast-conserving surgery with tumor less than 3 cm, have Estrogen Receptors (ER), and an age of 45 years and older. This revolutionary form of radiotherapy has given another option offering more room of convenience to patient.
4. Targeted therapy
Targeted therapy are treatments that target specific characteristics of cancer cells, for instance, a HER2 cancer type should be treated with HER2 targeted therapy, injected every three weeks for a year. In current treatment standards, Trastuzumab will be use in inhibiting at a single location, suitable for cases where no cancer has spread to the lymph nodes. In high-risk cases, where cancer has already spread to the lymph nodes, double targeting with two agent inhibitors such as Trastuzumab in combination with Pertuzumab, will be provided to maximize the effectiveness of the treatment.
5. Hormonal therapy
Hormone therapy is recommended to tumors that are hormone receptor-positive. Drugs like Tamoxifen should be considered as an adjuvant hormone treatment for cancer with Estrogen Receptors (ER), and Progesterone Receptors (PgR), which is applicable to both premenopausal and postmenopausal women. Aromatase inhibitors such as Letrozole, Anastrozole, and Exemestane are also available for postmenopausal women where these drugs inhibit the production of estrogen, such as stopping ovarian function in menstruation. The most commonly used hormone therapy such as Tamoxifen and Aromatase inhibitors should be taken one tablet every day for 5 years and an extended day up to 10 years for high-risk patient such as those whose cancer has spread to the lymph node.
Locally Advanced Breast Cancer (Stage 3)
In this stage of breast cancer, treatment is similar to the early stage breast cancer, however, surgery may not be the primary or the initial option of treatment as these tumors are larger or attached to nearby vital organs, such as a larger lymph node attaching to nerves and blood vessels. Surgery may not remove all cancers or may cause injury to nearby organs. Thus, most often, these cancers are treated with neoadjuvant chemotherapy (chemo before surgery) prior to surgery to shrink the tumor and making it easier to remove later in the surgery. Whereas other treatment such as radio therapy, targeted therapy and hormonal therapy follows similar indications with the early stage breast cancer.
Metastatic Breast Cancer (Stage 4)
The general aim of stage 4 cancer treatment is to alleviate symptoms with palliative care, stabilizing the metastatic disease, and prolong the patient’s life as much as possible. The main treatments for stage 4 breast cancer would be systemic therapies, or the use of drugs which may include chemotherapy, HER2 targeted therapy, or hormonal therapy. Each case will be treated differently based on the characteristics and types of cancer, metastasized organ, and patient’s physical and mental health condition. Currently, there are several new groups of drugs available; targeted therapy drugs such as CDK4/6 inhibitors, MTOR inhibitors, PI3K inhibitors or immunotherapy etc. Surgery and radiotherapy are not necessary in these group of patients unless under specific circumstances such as patient having a ruptured wound or have had initial aching pain. Besides cancer treatment, these cases also need to treat complications caused from breast cancer metastasizing to nearly any organ of the body. For example, if cancer has spread to the bone, symptoms may include aching in the bone, fractures, or even high calcium content in the blood.
By Assoc. Prof. Dr. Youwanush Kongdan
2414 New Petchaburi Road, Bangkapi, Hauykwang Bangkok 10310







 02-059-0245-48
02-059-0245-48 info@namarak.com
info@namarak.com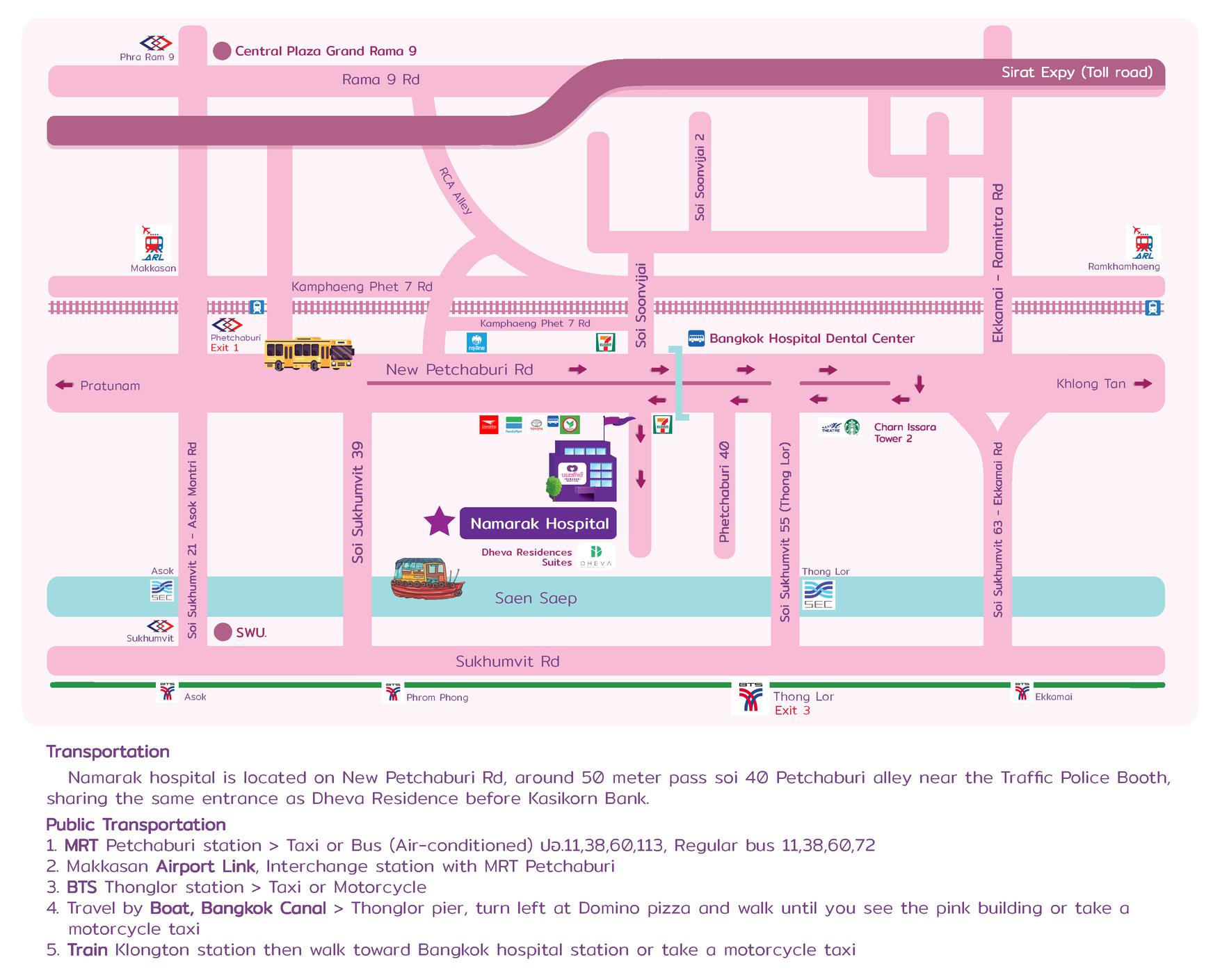 View Graphic Map
View Graphic Map Get Direction
Get Direction